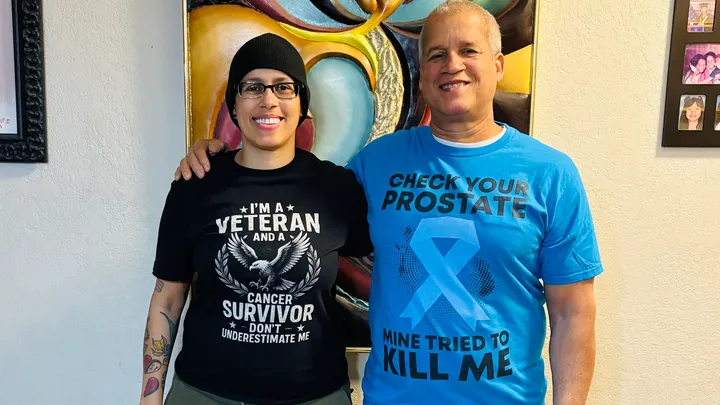
Power of Support During Dual Cancer Journeys
- A father and daughter were diagnosed with cancer just weeks apart, Eugenio with metastatic prostate cancer and Alicia with ovarian cancer, forcing them to navigate fear, treatment, and emotional shock together.
- Despite different diagnoses, both endured chemotherapy side by side, leaning on each other as doctors explained the challenges of advanced prostate and ovarian cancer
“Metastatic disease means that the cancer has left the prostate gland itself and has spread to other areas — specifically, the prostate cancer likes to go to lymph nodes, bones, or the lungs,” Dr. Neha Maithel, medical oncologist at UT Cancer Center in Houston, explains. - “For a man newly diagnosed with advanced prostate cancer, the number one treatment is going to be some type of systemic therapy, and in 2025, that is still almost certainly some type of hormonal therapy or drugs that block testosterone,” Dr. Daniel Hamstra, chair of radiation oncology at Baylor College of Medicine in Houston, tells SurvivorNet.
- Hormone therapy (Androgen Deprivation Therapy) is typically the first treatment for advanced prostate cancer, but when the disease learns to grow despite very low testosterone levels, it becomes metastatic castration‑resistant prostate cancer (mCRPC), which requires more advanced treatment approaches.
- Radioligand therapy is reshaping the way oncologists treat certain types of advanced prostate cancer — offering a highly targeted approach that delivers radiation directly to cancer cells while sparing surrounding tissue.
- “Ovarian cancer does not have any specific symptoms,” Dr. Beth Karlan, a gynecologic oncologist at UCLA Medical Center, explains, and adds it’s difficult to catch in its early stages due to vague symptoms like bloating, pelvic pain, and changes in bowel habits. Many cases begin in the fallopian tubes, with cancerous cells eventually spreading to the ovaries.
She considers her father one of the strongest men she knows, but the phone call delivering his diagnosis left her reeling.

“I remember waking up, and I got the phone call, and I wanted to break down my door,” she told WPLG News. “It was difficult.” “Metastatic disease means that the cancer has left the prostate gland itself and has spread to other areas — specifically, the prostate cancer likes to go to lymph nodes, bones, or the lungs,” Dr. Neha Maithel, medical oncologist at UT Cancer Center in Houston, explains. “Most people, when they have cancer, get very devastated about the news,” Eugenio said. “What really messes you up is the mindset.”
“For a man newly diagnosed with advanced prostate cancer, the number one treatment is going to be some type of systemic therapy, and in 2025, that is still almost certainly some type of hormonal therapy or drugs that block testosterone,” Dr. Daniel Hamstra, chair of radiation oncology at Baylor College of Medicine in Houston, tells SurvivorNet.
WATCH: Facing Prostate Cancer, What Will My Care Team Look Like?
In select cases, surgery may also be considered. Dr. Randall Lee, a urologic oncologist at Fox Chase Cancer Center, notes that “surgery in the advanced prostate cancer setting is a very nuanced discussion,” explaining that it may be an option when urinary blockage is present or when the cancer is locally advanced but hasn’t reached the lymph nodes.
As Alicia tried to support her father through his diagnosis, her own world shifted. Just one month later, she learned she had ovarian cancer.
“There are no words to describe what it feels like to watch your parent battle cancer while you’re fighting it yourself,” she wrote on GoFundMe.
“The fear. The exhaustion. The moments of strength followed by moments of complete heartbreak.”
When she received her diagnosis, she called the one person she knew would understand.
“I cried like a little baby to my dad,” she said. “He was the only person I cried to that I had cancer.”
WATCH: Women with a strong family history of ovarian cancer should talk to their doctor about genetic testing.
Ovarian cancer often begins in the fallopian tubes, where abnormal cells migrate to the ovaries and form tumors. The most common type typically appears around menopause, explains Dr. Beth Karlan of UCLA Medical Center.
“Ovarian cancer does not have any specific symptoms,” Dr. Karlan adds, which makes it difficult to catch in its early stages due to vague symptoms like bloating, pelvic pain, and changes in bowel habits.
Though their cancers are different, father and daughter share one grueling experience: both underwent chemotherapy as they fought their diagnoses side by side.
Going Through Chemo Together
“We are now halfway through our treatments and very hopeful. Our doctors are optimistic, and it truly looks like we are going to beat this. Every chemo session, every appointment, every hard day brings us closer to that finish line,” Alicia explained.
Chemotherapy is an effective tool for oncologists to help treat cancer by stopping cancerous cells from growing, dividing, and spreading to other organs. Chemo works by traveling through the bloodstream, killing cancerous cells. However, healthy cells are also impacted in the process, leading to side effects.

Patients almost universally experience fatigue, often alongside gastrointestinal side effects, such as nausea. Doctors have many effective medications to combat chemo-induced nausea. “But mitigating that fatigue often depends on the patient,” says Dr. Renata Urban, a gynecologic oncologist at the University of Washington in Seattle.
“Neuropathy is probably one of the most challenging side effects,” says Dr. Urban. Neuropathy results from damage to the peripheral nerves. It usually resolves after chemotherapy treatment, but sometimes symptoms can persist. While it’s typically characterized by numbness or a pins-and-needles sensation in the hands and feet, neuropathy can have several different symptoms, including:
- Weakness in the hands or feet
- Stabbing or burning pain in the hands or feet
- Difficulty gripping, such as when holding a fork
- Difficulty with fine motor skills, such as writing or buttoning a shirt
Nausea and vomiting are common side effects of chemotherapy. When chemotherapy affects the rapidly dividing cells in the lining of the stomach, the resulting cellular havoc in the gastrointestinal tract can lead to side effects such as nausea and vomiting. However, doctors can help patients mitigate the hit with various medications before, during, and after treatment.
“Part of the chemotherapy prescription includes a set regimen of anti-nausea medications,” says Dr. Urban. “We also ensure that patients have medications at home that they can use should they develop nausea after treatment.”
Hair loss is another side effect of chemotherapy.
WATCH: Coping with hair loss.
“For cancer patients, losing one’s hair can be unbelievably stressful. To start with, the dread of losing one’s hair can lead to some sleepless nights and feelings of anxiety,” Dr. Samantha Boardman, a New York-based psychiatrist and author, told SurvivorNet.
Most patients can expect regrowth four to six weeks after treatment. However, it is possible that when your hair grows back, you may notice some changes in its color and texture.
Tips for Navigating Chemo Side Effects
When dealing with fatigue, doctors don’t have an arsenal of weapons to combat fatigue in terms of prescription medications. However, you can do several things to help minimize the hit and restore your energy.
- Exercise: While it may be counterintuitive, physical activity can help alleviate side effects, especially fatigue. “Although ovarian cancer is not common, we often draw upon the experience of patients with breast cancer and colon cancer, who have shown that physical activity can not only improve quality of life but may also have beneficial impacts on cancer outcomes,” Dr. Urban says.
- Eat well: Even though nausea may interfere with your ability to eat a healthy diet, it’s essential to ensure you’re eating appropriately, getting enough protein, and not losing weight. Not only will nourishing your body support your recovery, but it may also help you feel more energized.
- Sleep: Want to mitigate fatigue? Be sure to maintain your regular sleep-wake cycle while on treatment. Sticking to a set sleep schedule helps reduce fatigue by ensuring enough hours for your body to heal and restore itself each night. It may also help you recover more quickly by keeping energy levels high during the daytime.
Digging Deeper Into Advanced Prostate Cancer Care
Prostate cancer, the most common cancer among men, begins in the walnut‑sized gland between the bladder and rectum that produces fluid to nourish sperm. Regular screenings often detect problems before symptoms appear. Treatment for advanced disease typically involves a combination of approaches, including hormone therapy, chemotherapy, immunotherapy, targeted therapy, or radiation.
For most men, hormonal therapy (androgen deprivation therapy) is the starting point for advanced prostate cancer care.
Hormone Therapy (Androgen Deprivation Therapy or ADT)
Prostate cancer cells grow in response to male hormones called androgens (mainly testosterone). Androgen Deprivation Therapy lowers androgen levels or blocks their effect, effectively starving the cancer. Men with intermediate or high-risk disease may turn to ADT for treatment.
ADT is a type of hormone therapy used to lower the levels of male hormones — called androgens — in the body. The main androgen is testosterone, which is produced mostly by the testicles. It is important because prostate cancer cells need testosterone to grow and survive.
WATCH: Are the Side Effects of Androgen Deprivation Therapy Worth the Risk?
By reducing or blocking testosterone, ADT can slow down the growth of cancer or even shrink it. ADT does not cure prostate cancer, but it is very effective at controlling it, especially when the disease is more aggressive or has spread beyond the prostate. In some cases, additional treatments are added to control the disease.
“We know that androgen deprivation therapy (ADT) alone, or lowering a man’s hormone levels through either shots or pills, are usually not enough to give them a long-term remission,” Dr. Gomella explains.
“We’ll usually add something else, such as a pill on top of the androgen deprivation therapy (ADT) to further weaken the cancer and improve a man’s outcome,” he adds.
Hormone levels may be lowered through:
- Injections or implants that stop testosterone production
- Pills that block testosterone from attaching to cancer cells
- Surgical removal of the testicles (this is less common today)
ADT often works well for years, but cancer can eventually adapt, leading to castration-resistant prostate cancer (CRPC). When that happens, additional treatments are used.
- Androgen Receptor Pathway Inhibitor (ARPI) Hormonal Agents
Drugs like abiraterone, enzalutamide, apalutamide, and darolutamide can further block androgen production or signaling, even after standard hormone therapy stops working.
“There are new, advanced hormonal therapies which are often combined with the traditional hormonal therapies,” Dr. Hamstra explains. “These are called androgen receptor blockers or ARPIs, and these can provide a more effective treatment, either in the castrate resistant setting or, frankly, in the castrate sensitive setting as well.” Indeed, in current practice, androgen receptor pathway inhibitors are commonly used in combination with traditional testosterone-lowering ADT for the majority of patients upon initial diagnosis of a metastatic prostate cancer.
- Chemotherapy
Medications like docetaxel or cabazitaxel target fast-growing cancer cells throughout the body. For some patients with advanced prostate cancer, chemotherapy can shrink tumors, ease symptoms, and improve survival. We’ll do a deeper dive into this further down.
- Targeted Therapy
If genetic testing of your cancer reveals certain mutations (for example, BRCA1/2), drugs like PARP inhibitors (olaparib, talazoparib, niraparib, rucaparib) may be effective.
- Immunotherapy
Some men with specific tumor markers (such as mismatch repair deficiency) may benefit from immune checkpoint inhibitors, which help the body’s immune system attack cancer, though Dr. Hamstra notes that the role of immunotherapy in prostate cancer treatment is not yet well-established. “Immune therapy has not played a huge role in prostate cancer at this point in time, but it is potentially something that may become more relevant,” he explains.
- Radiopharmaceuticals
These are radioactive medicines injected into the bloodstream that travel to metastatic sites and deliver targeted radiation, such as radium-223 or lutetium-177 PSMA therapy.
- Radiation Therapy for Symptom Control
External beam radiation can be directed at bone metastases or other symptomatic sites to relieve pain or prevent fractures.
- Clinical Trials
Participating in a research study can give access to cutting-edge treatments not yet widely available.
More on Chemo and Metastatic Prostate Cancer
“Chemotherapy definitely has a place in the treatment of many men with metastatic prostate cancer,” says Dr. Vivek Narayan, a medical oncologist at the University of Pennsylvania.
Dr. Narayan emphasizes that “not all chemotherapy is the same” and the type of chemotherapy used for prostate cancer is often better tolerated than the regimens used for other cancers, such as breast or lung cancer.
WATCH: Chemotherapy in Metastatic Prostate Cancer
“The chemotherapies that we conventionally use for prostate cancer can actually be better tolerated than some of the chemotherapies people may be familiar with. For example, the treatment of breast cancer, lung cancer, lymphomas, or other diseases that use a lot of chemotherapy,” Dr. Narayan said.
Since chemotherapy in prostate cancer tends to be better tolerated, Dr. Narayan says even older patients can often receive chemotherapy safely and effectively.
“We certainly have patients with prostate cancer, even in the older ages, seventies and even eighties, who we successfully give chemotherapy to. So, it can be done. There is a trade-off.”
When Is Surgery Used For Advanced Prostate Cancer? What Patients Should Know
For many men facing an advanced diagnosis, surgery will not be part of the treatment plan; however, there are certain situations where it can be beneficial.
Dr. Randall Lee says the possibility of surgery “depends on the patient, and it requires a lot of discussion and counseling.”
If the prostate cancer has only spread to a few spots — or what doctors call oligometastatic disease — hormone therapy, also known as androgen deprivation therapy (ADT), along with local radiation therapy, is typically the first choice for control.
WATCH: When Is Surgery Used For Advanced Prostate Cancer?
However, if the patient is dealing with urinary blockage or if the cancer is locally advanced but hasn’t spread to the lymph nodes, Dr. Lee points out that surgery could be an option for some of these patients.
Weighing Risks & Benefits
Surgery in advanced prostate cancer isn’t always straightforward. There can be side effects and risks from anesthesia, and it’s important to weigh how the procedure might affect your quality of life while still keeping the cancer in check. That’s why doctors take extra care in deciding who’s a good fit for surgery.
“In the appropriately selected patient that is counseled on the risks and benefits of surgery… it is possible, and it’s definitely something that is offered,” Dr. Lee explains.
When it comes to prostate cancer surgery, there’s no one-size-fits-all approach. One option is a prostatectomy, where the surgeon removes the entire prostate along with some surrounding tissue, including the seminal vesicles (they help produce semen). This procedure is usually considered for patients whose cancer hasn’t spread beyond the prostate.
It’s important to know that a prostatectomy can come with side effects, like erectile dysfunction or urinary incontinence, which is why doctors weigh the pros and cons carefully before recommending it.
WATCH: Preparing For Prostate Cancer Surgery: Before, During & After
It can be performed using two primary approaches: open radical prostatectomy or minimally invasive (robot-assisted laparoscopic) prostatectomy. While both robotic and open prostatectomy can offer excellent cancer control, robotic-assisted surgery has emerged as the preferred method for its potential advantages in recovery time, pain, and preservation of urinary and sexual function.
Surgery also doesn’t always mean removing the whole prostate. In some cases, especially for patients dealing with urinary issues or going through radiation, doctors might suggest procedures similar to those used for BPH (benign prostatic hyperplasia) — that’s when the prostate is enlarged. These surgeries help open up the urinary tract.
“There are surgeries in which we are able to open up the urinary tract to allow patients to have a better quality of life so they don’t run into issues after radiation or during radiation,” Dr. Lee explained.
If you’re facing advanced prostate cancer, the most important thing is to talk openly with your care team. Don’t hesitate to ask about all your options—including whether surgery makes sense for you. And make sure your personal concerns, like how treatment might affect your urinary symptoms, sex life, or your long-term quality of life, are part of that conversation.
Understanding Prostate Cancer Recurrence
Prostate cancer recurrence is not all that uncommon. A study published in the medical journal JAMA followed 1,997 men who had undergone prostate removal surgery. Of those, 304 experienced a recurrence, and about 25% of those cases occurred five or more years after surgery.
Researchers believe that dormant cancer cells can hide in the body for years. The bone marrow, in particular, is considered a key hiding place. This is supported by findings published in the International Journal of Cancer, which noted, “In one autopsy study, approximately 80% of the men who had died from prostate cancer possessed bone metastases.”
Other potential reservoirs for dormant cancer cells include the lymph nodes and the prostate bed—the area where the prostate gland once was—though these are more difficult to study.
Researchers have made significant strides in understanding how prostate cancer can spread early—even when it appears to be under control—and then return months or even years later. One key discovery is that the bones are a common site for prostate cancer to spread. In fact, scientists have found dormant cancer cells hiding in the bone marrow of many patients, even when the disease seems confined to the prostate.
Lab studies, mostly using model systems, have also helped uncover how prostate cancer cells can lie dormant for long periods before becoming active again. While treatments like hormone therapy and radiation after surgery have shown promise, experts agree that more research—both in the lab and in clinical trials—is needed to improve outcomes for patients.
Prostate Cancer Screening and Warning Signs
When you do get screened for prostate cancer, your doctor will run a few tests.
One of the tests is the PSA test, a simple blood test that screens for prostate cancer. It looks for more significant amounts of protein-specific antigen (PSA) in the blood. An elevated PSA test does not always mean you have prostate cancer. It could also reflect that your prostate is enlarged, which is common, or it could signal an infection or inflammation.
Your doctor may also conduct a digital rectal exam (DRE) to check your prostate for lumps.
Depending on the results of these tests, imaging scans and a biopsy may be ordered.
WATCH: How Gleason Grade Determines Treatment
Prostate cancer does not always behave the same in every man it impacts. The cancer can be considered “low-risk” and can be slow-growing, and treatment might not be necessary. In other men, the cancer may grow faster or more aggressively, requiring more immediate treatment. Because of this, there is some debate about screening.
The United States Preventive Services Task Force recommends that men at average risk between the ages of 55 and 69 years talk with their doctor about the pros and cons of prostate cancer screening.
The American Cancer Society recommends that men at age 50 who are at average risk should begin screening. Men who are at high risk of prostate cancer should begin screening at age 40. Men with a close relative diagnosed with prostate cancer should consider annual screenings in their 30s.
SurvivorNet experts suggested that men consider factors like their family history, genes, and age when deciding whether and when to screen.
Symptoms of prostate cancer may include:
- Urinating more often
- Waking up in the middle of the night to pee
- Blood in your urine
- Trouble getting an erection
- Pain or burning when you urinate
- Pain in your back, hips, thighs, or other bones
- Unexplained weight loss
- Fatigue
Understanding an Ovarian Cancer Diagnosis
Ovarian cancer has been called the “cancer that whispers” because women often don’t experience symptoms until their cancer has already reached its late stages. The symptoms that do appear at first are hard to identify as cancer.
“Ovarian cancer does not have any specific symptoms,” Dr. Karlan explained.
The symptoms of ovarian cancer may include the following, according to SurvivorNet experts.
- A feeling of bloating or fullness
- Pain in the pelvis or abdomen
- Nausea
- Vomiting
- Changes in bowel habits
WATCH: Fighting “Platinum Resistant” Ovarian Cancer
On the horizon is a treatment option for patients with platinum-resistant ovarian cancer. Platinum resistance is typically defined as progression within 6 months of receiving platinum-based chemotherapy. The Phase III ENGOT‑ov65/KEYNOTE‑B96 trial has shown great promise for this difficult-to-treat form of ovarian cancer, exploring adding immunotherapy, where the patient’s own immune cells are reengineered to fight cancer, to chemotherapy.
Dr. Premal Thaker, a gynecologic oncologist at Washington University, recalls, “We all know, checkpoint inhibitors have made a big splash in many cancers, and we have been trying so hard in ovarian cancer to try to use these immune checkpoint inhibitors…”
For patients whose tumors had a PD-L1 (a protein on the surface of some cancer cells) CPS combined positive score (measuring how much PD-L1 a tumor expresses) of 1 or higher, treatment with pembrolizumab helped them go longer without cancer progression. Their median progression-free survival was 8.3 months compared with 7.2 months for those who received a placebo, a difference that was statistically meaningful.
Dr. Robert Coleman, a gynecologic Oncologist at Texas Oncology in Houston, remarks, “We saw no new adverse events outside our expectations, nor did we see an acceleration of adverse events with the combination, including the triplet.”
Dr. Coleman explains, “In the platinum-resistant setting, I believe these will be favored regimens, so as a second-line therapy…Ultimately, cross-trial comparisons will drive some of the influence of those trials and the sequencing of therapy. This will likely be further augmented by biomarker expression, which we expect to be more robust as time goes on.”
With regard to how this treatment may fit in with other systemic options, such as antibody drug conjugates, Dr. Dana Chase, a professor of gynecologic oncology at UCLA Health, explains, “The sequencing of the treatment is really dependent on the patient’s tumor biomarker profile. We will need to take into consideration: 1) biomarker profile, 2) prior toxicities, 3) patient’s performance status, and/or goals of care/treatment. Depending on these three factors, we may either treat with an ADC first or choose options like the B96 option first.”
Dr. Chase adds that, “The sequencing of the treatment is really dependent on the patient’s tumor biomarker profile. We will need to take into consideration: biomarker profile, prior toxicities, patient’s performance status, and goals of treatment.” Depending on those three factors, doctors can best decide which treatment to pursue first.”
The Standard of Care for Ovarian Cancer
The standard of care for ovarian cancer patients is chemotherapy, which helps many patients reach remission.
WATCH: How your ovarian cancer responds to certain types of chemotherapies guides your future treatments.
With recurrence a strong possibility for this disease, especially in the later stages of ovarian cancer, certain drug treatments to deal with it are giving many women hope.
Maintenance therapy is continued treatment after the patient finishes their initial treatment. After an ovarian cancer patient completes a round of treatments — such as surgery and chemotherapy — her doctor may recommend some form of maintenance therapy to try and delay possible recurrence. Maintenance therapy can involve taking an oral pill called a PARP inhibitor every day after chemotherapy and can keep cancer in remission longer.
Genetic testing helps doctors determine the best maintenance therapy.
The type of treatment recommended for recurrence can depend on several factors:
- The period within which the cancer recurred
- The kind of chemotherapy the woman underwent in the past
- Side effects that came as a result of past treatments
- The length of time between the last treatment the woman underwent and the recurrence
- The specific mutations and molecular features of your cancer
What’s the Standard of Care for Ovarian Cancer Recurrence?
Ovarian cancer returning after initial treatment is common; in fact, recurrence happens in “almost 25 percent of cases with early-stage diseases and in more than 80 percent with more advanced stages,” according to research published in the Gland Surgery medical journal.
For many women, platinum-based chemotherapy—often the first line of defense—remains effective across multiple cycles. But over time, cancer cells may adapt, and resistance can emerge after just one round or several.
Platinum Sensitivity vs. Resistance: What It Means for Treatment
- Platinum Sensitive: If a patient remains cancer-free for more than six months after platinum therapy, they’re considered platinum sensitive. This signals that the cancer is still responding, and doctors may continue using platinum-based drugs.
- Platinum Resistant: If recurrence occurs within six months, the cancer is classified as platinum resistant. In these cases, oncologists typically shift to alternative therapies tailored to overcome resistance.
Adjusting Chemotherapy Strategies
- Taxol (Paclitaxel): Commonly paired with platinum in initial treatment. For platinum-resistant patients, doctors may increase its frequency—administering it weekly instead of every three weeks.
- Other Options: Drugs like Gemzar (gemcitabine), Topotecan, and Doxil (liposomal doxorubicin) are often introduced, sometimes alongside Avastin (bevacizumab).
How Avastin Works
Avastin is a VEGF inhibitor that blocks angiogenesis—the process by which tumors grow new blood vessels. By cutting off this supply, Avastin helps starve the tumor and slow its progression. It’s frequently combined with chemotherapy in recurrent cases.
Targeting DNA Repair: Platinum & PARP Inhibitors
- Platinum drugs and PARP inhibitors share a powerful mechanism: they disrupt a cancer cell’s ability to repair damaged DNA. This is especially effective in patients with BRCA mutations, whose cells already have impaired DNA repair pathways.
- PARP Inhibitors: Initially tested in BRCA-positive patients with recurrent ovarian cancer, these drugs are now used more broadly. Emerging evidence shows they can extend survival even in patients without BRCA mutations.
- Genetic Testing: Oncologists strongly recommend BRCA testing for all ovarian cancer patients. Knowing your genetic profile helps guide treatment and opens doors to targeted therapies.
Questions for Your Doctor
If you have been diagnosed with ovarian cancer and need guidance to further educate yourself on the disease and treatment, consider these questions for your doctor.
- What type of ovarian cancer do I have?
- What stage is my cancer in?
- Do you recommend I get genetic testing for any gene mutations, such as the BRCA gene mutation?
- What initial treatment options do you recommend?
- What are the possible side effects of the recommended treatment, and how can they be coped with?
- Will insurance help cover my recommended treatment?
Learn more about SurvivorNet's rigorous medical review process.